UnitedHealthcare Just Cut Prior Auth by 30%. Here’s What That Actually Changes.
Written by Emily Davis

UnitedHealthcare Just Cut Prior Auth by 30%. Here's What That Actually Changes.
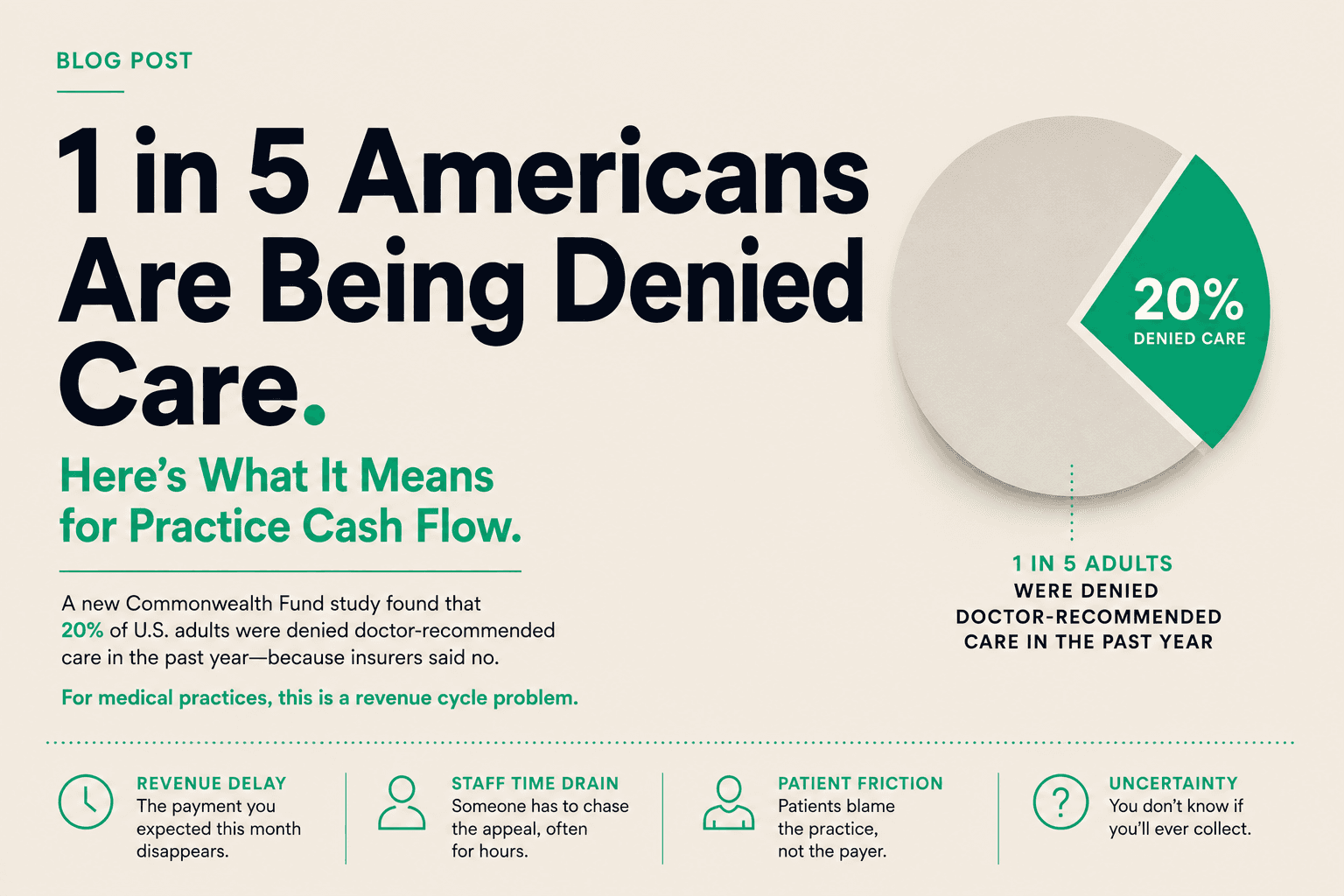
UnitedHealthcare announced last week that it will eliminate an additional 30% of remaining prior authorization requirements by the end of 2026. Outpatient surgeries. Diagnostic tests like echocardiograms. Gone from the auth queue.
It is the kind of headline that looks like a win. For some practices, it will be. But the full picture is worth reading carefully, because what changes and what does not change matters more than the number.
What UHC is actually doing
UnitedHealthcare has been trimming its prior auth list for a couple of years. The latest cut is the largest announced in a single move. Thirty percent of remaining requirements is a meaningful reduction, particularly in outpatient surgery and diagnostics, where authorization delays have historically caused the most disruption to scheduling and patient care.
The categories being removed are not random. They tend to be high-volume, lower-complexity procedures where the clinical justification is consistent and the denial rate on initial review was low. In other words, UHC is cutting the authorization requirements that were generating the most friction for the least legitimate gatekeeping purpose.
That is the right call. It also reveals something worth sitting with: a significant portion of the prior auth burden that practices have been managing for years was never clinically necessary. It was administrative inertia.
What does not change
Here is the part that gets lost in the headlines. Eliminating prior authorization for a procedure is not the same as eliminating the payment lag.
When UHC removes an auth requirement for echocardiograms, your cardiology practice no longer has to request approval before scheduling. That saves time, reduces friction, and means fewer patients wait weeks for a test. Real improvement.
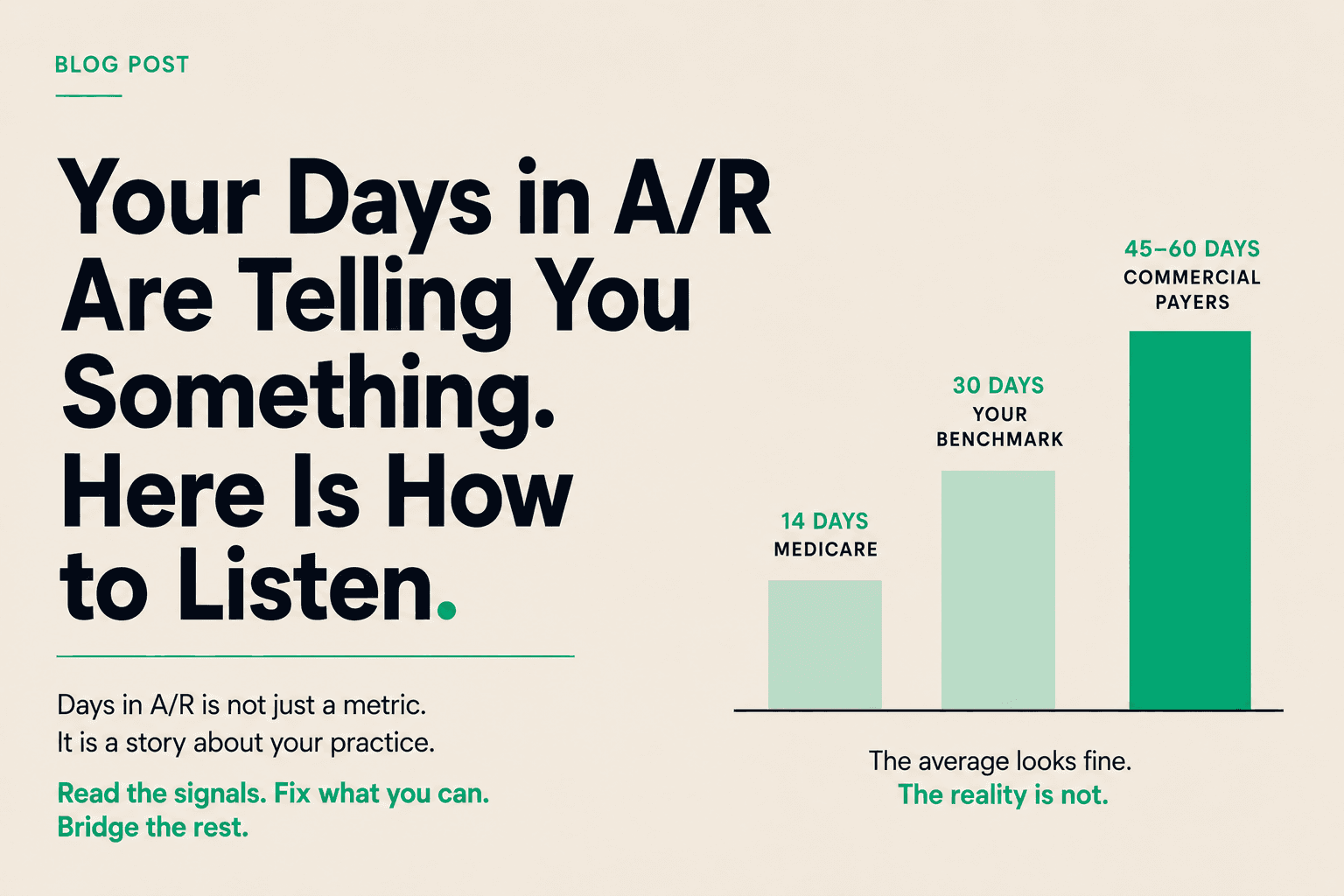
But the claim for that echocardiogram still enters UHC's payment processing queue. It still sits there for 30 to 45 days while their system reviews, adjudicates, and issues payment. The prior auth step that used to add 5 to 10 days to the front of that process is gone. The payment timeline that follows has not changed.
For practices measuring their cash flow impact, the gain is real but partial. You still get paid on UHC's schedule. It is just now a UHC schedule that does not include a detour through the authorization desk.
The MA auto-enrollment proposal
There is a separate development worth watching alongside the UHC announcement. Forbes reported this week that the Trump administration is considering auto-enrolling newly eligible Medicare beneficiaries into Medicare Advantage plans or Accountable Care Organizations, rather than defaulting them into traditional Medicare.
The implications for independent practices are significant. If auto-enrollment moves forward, the MA enrolled population grows faster than it would through voluntary sign-up. More patients arrive at your practice on MA plans. More claims go through MA payer systems, which have historically been slower to pay and more aggressive on authorization than traditional Medicare.
The Forbes analysis also flags the risk to patients: narrower networks and more prior authorization requirements compared to traditional Medicare. For practices already managing MA complexity, a larger MA-enrolled patient base means more volume running through the part of the payer system that generates the most cash flow friction.
Nothing is final on auto-enrollment yet. But the direction matters for planning. If your practice has been gradually absorbing more MA volume over the past few years, the trend is likely to continue regardless of policy changes, and may accelerate.
Independent evidence and denial rates
One more data point from last week: a Forbes analysis of independent evidence reviews in New York found that large numbers of insurance denials were overturned when independent clinical experts reviewed the cases. The overturn rate was high enough to suggest that a substantial portion of current denial volume is not based on clinical evidence. It is based on default denial workflows that assume most practices will not appeal.
This matters for two reasons. First, if you are not appealing denials systematically, you are leaving money on the table. Second, it confirms what many practice administrators already suspect: the prior auth and denial system as currently designed is partially a cash flow management tool for payers, not a clinical gatekeeping function.
UHC cutting 30% of auth requirements is a real step. The underlying structure — where payers control both the timing of approvals and the timing of payment — is unchanged.
What to do with this
The operating reality for independent practices this week is not dramatically different from last week. Auth friction is going to decrease for some procedures. The payment lag persists. MA enrollment may grow faster than expected. Denials still need to be appealed.
The practices in the best position are not waiting for the system to finish reforming before they address their cash flow structure. They are treating A/R as a tool now, building the muscle of accessing capital from submitted claims rather than waiting on payer timelines that shift slowly and unpredictably.
Prior auth reform is welcome. It is not the same as getting paid faster. Understanding that distinction is the starting point for building a practice that does not depend on payer reform to run well.