Prior Authorization Is Not Your Cash Flow Problem. The Gap Behind It Is.
Written by Emily Davis

Prior Authorization Is Not Your Cash Flow Problem. The Gap Behind It Is.
Most independent practice owners talk about prior authorization like it is the core issue. Get the authorization faster, the thinking goes, and the money flows.
That is partly true. But authorization is the trigger, not the constraint.
The real problem is the gap. The time between when you complete the work and when the payer settles the claim. Prior auth is one contributor. Payment processing timelines are another. Claim review queues. Secondary manual review flags. Denial appeals that restart the clock.
Authorization reform, when it eventually arrives, will help. But it will not close the gap. And independent practices need to understand what the gap actually costs them.
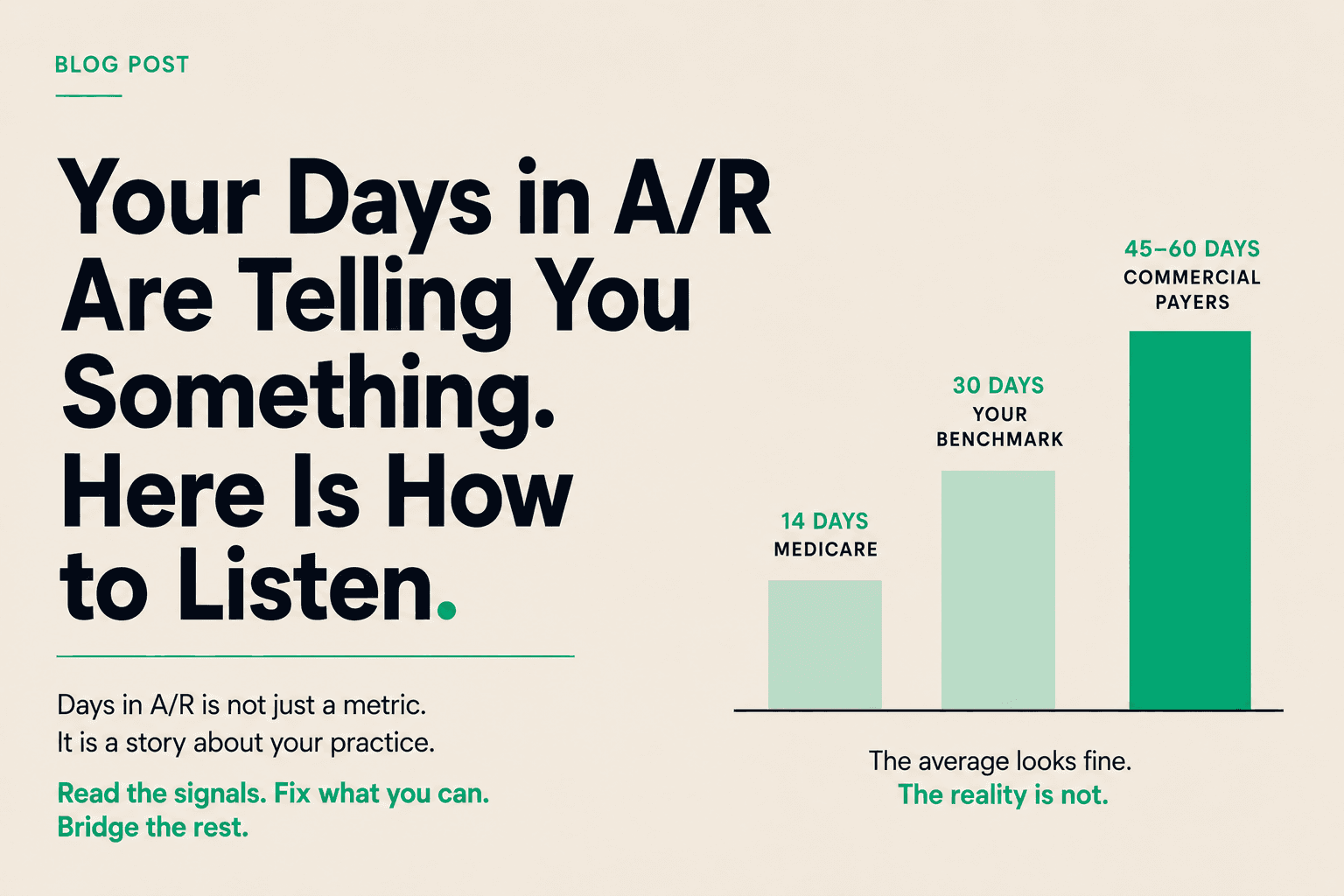
What the gap looks like in numbers
Here is a simplified version of how the cash flow math works for a primary care practice generating $800,000 a month in claims.
Say you have a 60-day average payment cycle. That means at any given moment, you have roughly two months of revenue sitting in A/R that is submitted but unsettled. On $800,000 per month, that is $1.6 million in receivables that exist on paper but not in your operating account.
Your payroll is probably $80,000 to $120,000 a month. Your rent, supplies, and overhead add another $60,000 to $100,000. Every month you cover $140,000 to $220,000 in operating costs against cash that lags your revenue by 60 days.
That is manageable if your cash reserves are healthy and your collections are consistent. It becomes a problem when claims hit friction, when volumes shift, when a new service line creates a ramp-up period, or when you want to grow.
Why prior auth reform will not fix this
CMS proposed the electronic prior authorization rule for Part B drugs this year. Cigna says 70% of its prior auth volume will be standardized electronically by end of 2026. These are real improvements.
But authorization is a gate. Even if the gate opens faster, the payment timeline runs on a separate clock. A prior auth that takes one day instead of five days still results in a claim that sits in the payer's processing queue for another 30 to 45 days.
Electronic standardization means electronic submission. It does not mean instant approval. It does not mean instant payment. The gap shrinks at the authorization stage but persists at the payment stage.
For practices in specialties with high auth volume, this matters. You may run tighter auth workflows next year. You will still be waiting on the same payer timelines.
The three tools practices use to manage the gap
Most practices use some combination of three approaches.
Cash reserves. Build up enough operating cash to absorb the lag comfortably. This works until you want to grow, hire, or expand, at which point the reserve gets consumed by the upfront cost and the gap gets longer before it closes.
Credit. A line of credit, an equipment loan, a practice acquisition loan. Useful for specific capital needs but adds debt service to margins that are already thin. Lenders want collateral and multi-year commitments that limit flexibility.
Ignoring it. A surprising number of practices do not explicitly model the gap. They know cash is tight sometimes. They do not trace it to specific payer timelines. This makes it harder to fix because you cannot optimize what you have not measured.
There is a fourth option.
Treating A/R as a liquid asset
Your submitted claims are assets. They represent work already done and money already owed. The payer's payment timeline is not your timeline. It is the timeline the payer has set for their own cash management.
Healthcare receivables financing lets you access a portion of the value of submitted claims before the payer settles. Not a loan. Not factoring that involves selling your receivables at a discount and losing control of your billing relationship. An advance tied to specific claims, at the claim level, at a transparent per-diem rate.
When the payer settles, the advance reconciles. You paid a small, predictable cost for the use of capital during the gap period. The gap still exists. You just stopped waiting in it.
At Copay, the rate is 0.75% for the first 10 days, with a daily rate after that. If your payer settles in 15 days, you know exactly what it cost. No minimums. No contracts. No impact on your billing operations.
Who this changes the math for
Healthcare receivables financing is not for every practice. It makes the most sense when:
You have consistent patient volume and solid clean claim rates
Your gap is 30 days or longer with commercial payers or Medicare Advantage
You are leaving growth on the table because capital is not available at the right moment
You have looked at a line of credit and do not want the commitment
The practices getting the most out of this tool are not using it because they are struggling. They are using it because they have learned to treat their A/R as a tool, not a waiting room.
The bottom line
Prior auth reform will help. It is real progress. But the cash flow gap is not primarily an authorization problem. It is a structural feature of how healthcare is paid for in the United States.
Understanding the gap, modeling what it actually costs your practice, and having a tool to work around it is not optional anymore for practices that want to grow. It is table stakes.
If you want to run the math on what the gap costs your practice and whether receivables financing makes sense at your volume, Copay is a good place to start.