Health Systems Are Walking Out on Medicare Advantage. Independent Practices Are Next in Line.
Written by Emily Davis

Health Systems Are Walking Out on Medicare Advantage. Independent Practices Are Next in Line.
Twenty-one health systems have now dropped at least one Medicare Advantage plan in 2026. The number keeps climbing. Every single one cites the same two reasons: prior authorization denials and slow reimbursement.
When a health system with a legal team, a CFO, and leverage over payer negotiations decides a contract is not worth it, that tells you something. It tells you the administrative burden and payment friction have crossed a line that the volume cannot justify.
Now think about what happens next.
The patients go somewhere
Health systems are not the end of the line. When HCA or CommonSpirit exits a Medicare Advantage network, the patients on those plans do not disappear. They migrate. In many markets, that migration flows to independent practices that remain in-network with the same MA plans.
Those practices do not have legal teams reviewing contract terms. They do not have leverage to renegotiate. They absorb whatever the plan's prior authorization requirements and reimbursement timelines say, because exiting the network is not a real option for a three-physician group dependent on that patient volume.
This is the downstream effect nobody is talking about. The administrative churn that large systems decided was unsustainable gets redistributed to providers with less capacity to manage it.
The MA benefit cuts are coming
Reuters reported this week that Medicare Advantage plans are preparing to cut supplemental benefits in 2027. Humana has been offering more in 2026 than its rivals. That gap is going to close.
This matters for patient volume and payer mix. When MA benefits get cut, some patients rethink their plan choices during open enrollment. Others stick with their plan and simply lose coverage for services they used to have. For practices that built patient volume around MA enrollees, the mix is shifting.
None of this is catastrophic on its own. But add it to the trajectory. MA plans are under financial pressure. They are responding by cutting benefits and tightening authorization. Health systems are exiting. The burden redistributes.
The standardization promise has a gap
Here is the nuance. Cigna announced it expects 70% of prior authorization volume to be standardized electronically by the end of 2026. Other large payers are making similar moves.
That sounds like progress. It is, partly. Electronic prior auth is faster and less chaotic than faxing. But 70% standardized means 30% still is not. And even standardized electronic auth does not mean faster approval. It means faster submission. The denial rates and the manual review triggers are separate from the workflow infrastructure.
A Forbes piece published today analyzed independent evidence reviews in New York and found that large numbers of insurance denials were overturned when independent clinical experts got involved. The overturn rate was high enough to suggest that a significant portion of current denial volume is not based on clinical evidence.
If denials are getting overturned at scale when someone actually reviews them, that means practices submitting clean claims on legitimate services are still waiting, still appealing, still absorbing the cash flow gap created by a process that is slow by design.
The WISeR wrinkle
CMS launched the WISeR model this year in six states: New Jersey, Ohio, Oklahoma, Texas, Arizona, and Washington. It is a voluntary model encouraging providers to navigate toward evidence-supported care for Medicare patients, with prior authorization framed as the quality gate.
For practices in those states, this is another layer of documentation and review. The upside is that CMS is at least trying to build a framework where prior auth has a clinical rationale rather than a financial one. The downside is transition periods always create friction before they create clarity.
What practices do with this
The common thread in all of this: the gap between delivering care and getting paid is not narrowing. The mechanisms are changing, some of the infrastructure is improving, but the underlying cash flow exposure is the same.
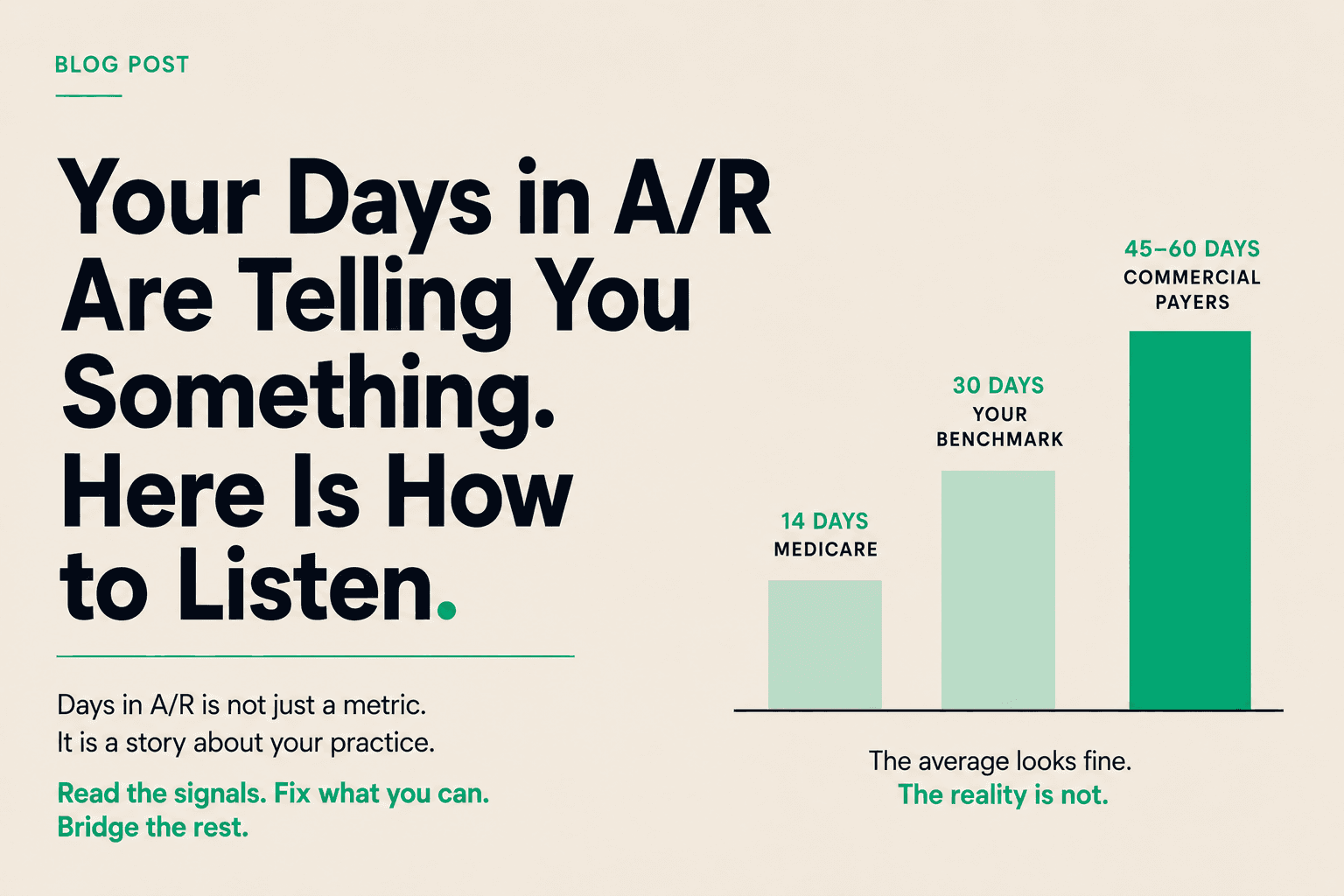
You see a patient. You submit a claim. The payer sits on it for 30, 60, sometimes 90 days. Prior auth delays push that out further. Denials restart the clock. And your payroll, rent, and supplier invoices do not wait.
The practices managing this best are not waiting on policy reform or payer goodwill. They are treating their submitted claims as working capital and accessing that capital before the payer settles.
That is what Copay does. Turn your A/R into a tool you can use, not a number you watch.
If the MA exodus is landing additional administrative weight on your practice and your cash position is showing it, we should talk.