Three Headlines, One Problem: What This Week in Healthcare Means for Independent Practices
Written by Emily Davis

Three Headlines, One Problem: What This Week in Healthcare Means for Independent Practices
Three things happened in healthcare policy this week that, on the surface, look unrelated. Dig in and they are all telling the same story.
The payment system is getting harder to navigate. The cash flow gap is getting wider. And independent practices are absorbing the cost.
Here is what happened, and why it matters.
Story One: Health System CEOs Blink on Site-Neutral Payments
On Tuesday, the CEOs of some of the largest health systems in the country sat in front of a House committee and said something nobody expected: they are open to discussing site-neutral payment reform.
Site-neutral payments would require Medicare to reimburse the same service at the same rate regardless of where it is performed. Right now, a hospital outpatient department gets paid significantly more for the same procedure than an independent practice or ambulatory surgery center. It is a major reason hospitals have spent the last decade buying up physician practices. Once you are a hospital-affiliated provider, your rates go up without changing a single thing about the care you deliver.
The hearing got pointed fast. GOP lawmakers accused health systems of driving costs and limiting competition. Democrats focused on cuts in the current reconciliation bill. But the real news was the concession: executives from HCA, CommonSpirit, and New York-Presbyterian signaled they were willing to give ground.
What does this mean for independent practices? Two things.
First, if site-neutral payments expand, independent practices become less attractive acquisition targets. That sounds like good news for independence, and it is, except that it does not solve the underlying financial pressure that makes selling to a health system tempting in the first place.
Second, this debate reveals how much of the reimbursement disparity in Medicare has been built around facility fees, not clinical value. Independent practices have been competing in a system where the pricing rules favor consolidation. That may start to change, but the transition will be slow and messy, and the cash flow constraints will remain in the meantime.
Story Two: 21 Health Systems Are Dumping Medicare Advantage
According to a running tracker from Becker's, 21 health systems have severed ties with at least one Medicare Advantage plan in 2026. The reason cited every single time: prior authorization denials and slow reimbursement.
The scale of this tells you something. These are not small regional hospitals making a tactical move. These are major systems with leverage and legal teams deciding that the administrative burden and payment delays from MA plans are not worth the volume.
Now think about what happens to those MA patients. They do not disappear. They go somewhere. In many cases, that somewhere is an independent practice that is in-network with those same plans, operating with far less margin for absorbing claim friction.
MA plans denied 4.1 million prior authorization requests in 2024, a 7.7% denial rate. When health systems exit MA networks, the administrative churn of managing those patients and their prior auth requirements does not vanish. It redistributes. And independent practices are downstream of that redistribution.
At the same time, Congress introduced the Medicare Advantage Improvement Act of 2026 this week. Bipartisan bill, co-sponsored by a group of physician-legislators. It would tighten oversight of MA plans, curb retroactive denials, and require that approved claims get paid promptly.
The intent is right. But federal legislation takes time. In the meantime, practices are dealing with the denial rates and payment delays that exist today.
Story Three: CMS Wants to Extend Electronic Prior Auth to Drugs
On April 10, CMS released a proposed rule that would extend the electronic prior authorization framework to drugs billed under the medical benefit, specifically provider-administered therapies under Medicare Part B.
This is the first time federal policy has proposed requiring electronic prior auth for these drug categories. The public comment period closes June 15. If the rule is finalized, payers would need to build drug coverage requirements into their prior authorization APIs by October 1, 2027.
For specialty practices, the ones billing injectables, biologics, and infusion therapies, this is a double-edged development. The mandate for electronic workflows is genuinely useful. Manual, paper-based prior auth for high-cost biologics is a genuine mess. Practices that are still faxing prior auth requests know exactly what that costs in staff time and delayed care.
But the compliance timeline is tight and the transition period creates risk. Until payers fully implement these APIs, practices running specialty drug protocols will face a period where the old workflows are eroding and the new ones are not fully operational. That is a cash flow exposure window.
The proposed 24-hour turnaround requirement for some drug prior auth decisions under Medicaid is genuinely aggressive. If it holds, it would meaningfully reduce the auth-to-treatment delay in high-cost specialty care. But turnaround requirements and actual payer behavior are not always the same thing.
What These Stories Add Up To
Take a step back and you get a consistent picture.
The site-neutral debate signals that the reimbursement structure favoring hospital-employed physicians is under serious pressure. But structural change in Medicare policy takes years.
The MA exodus by health systems signals that prior auth burden and payment delays have become unsustainable even for organizations with significant leverage. For independent practices with less leverage, those same frictions are equally real and harder to manage.
The drug prior auth reform signals that CMS is aware the current system creates administrative drag. But the window between proposal and operational implementation is exactly the kind of period where claims back up and cash flow gets unpredictable.
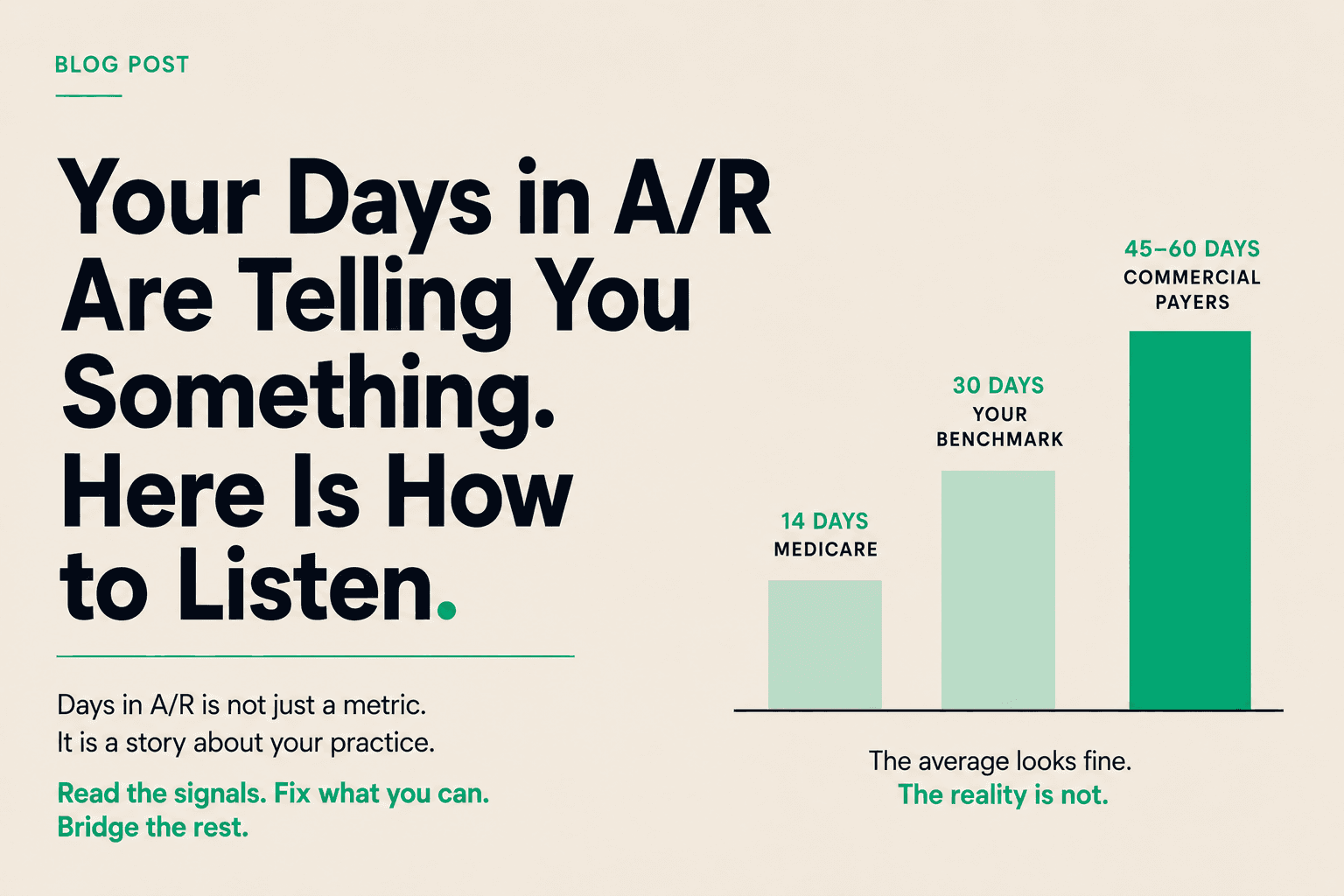
None of this resolves in the next quarter. Independent practices navigating this environment need to treat their A/R as an active asset, not a passive waiting game.
Where Copay Fits
Every story this week is a cash flow story at its core.
Site-neutral reform, if it happens, will disrupt how practices are valued and create a transition period of payment uncertainty. MA plan upheaval redistributes prior auth burden and payment risk onto providers with less infrastructure to absorb it. Drug prior auth reform opens a compliance window that delays reimbursement cycles on high-cost specialty services.
Copay works with independent practices to access the value of submitted claims before the payer settles. Not a loan, not factoring. Advances tied to specific claims, at a simple transparent cost, with no long-term contracts.
When the policy environment is this volatile and payer timelines are this unpredictable, having a tool that disconnects your cash position from the payer's timeline changes what your practice can do.
The practices navigating 2026 well are not the ones waiting on policy reform. They are the ones who stopped waiting on reimbursement.