CMS Prior Auth Rule Takes Effect July 1: What Practices Actually Need to Know
Written by Emily Davis

CMS Prior Auth Rule Takes Effect July 1: What Practices Actually Need to Know
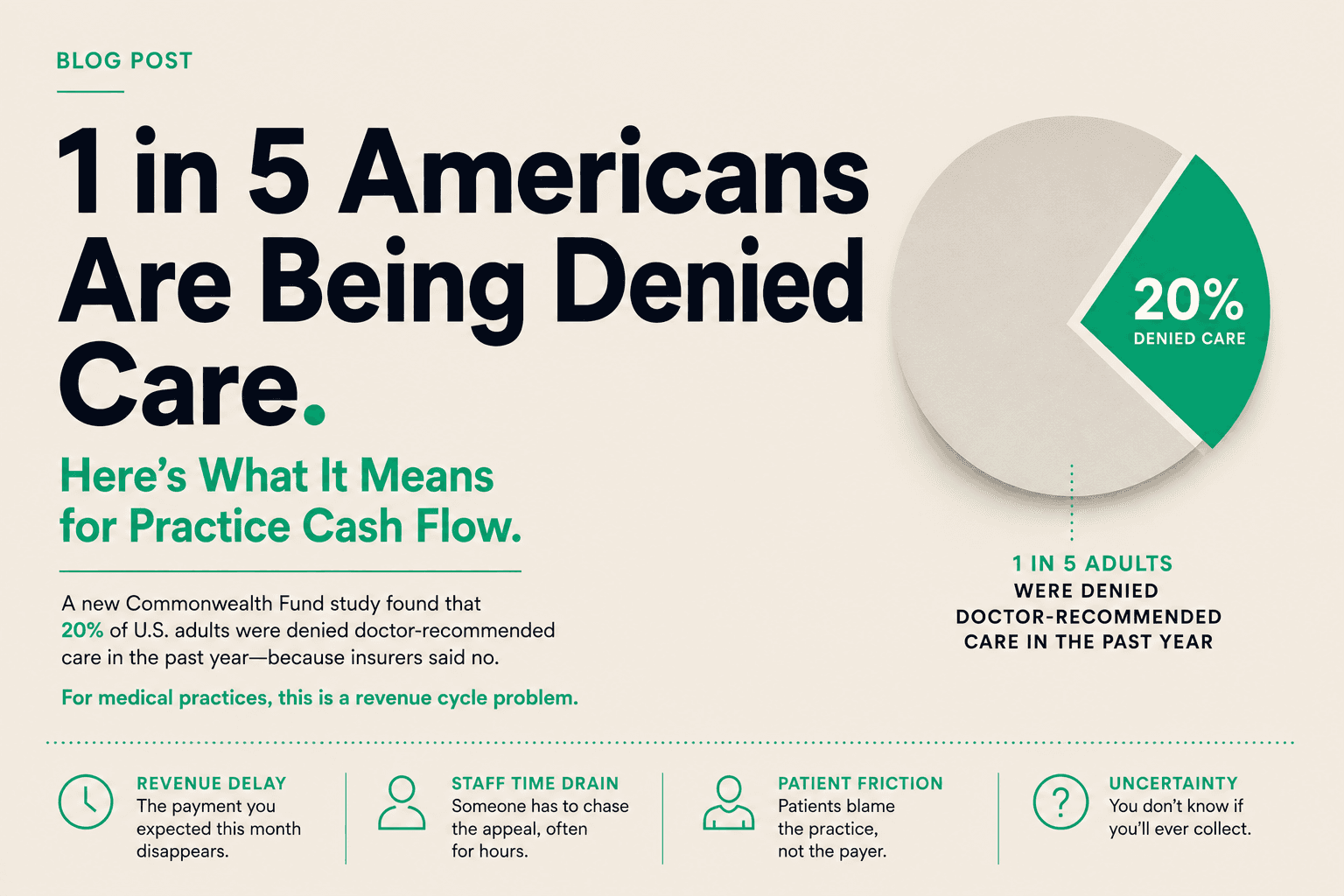
The CMS prior authorization rule for Medicare Advantage and Medicaid managed care goes into effect July 1, 2026. This is the rule that has been discussed, debated, and delayed for over a year. It is finally here.
Here is what it actually requires, what it does not cover, and what independent practices should do about it.
What the rule requires
Starting July 1, MA and Medicaid managed care plans must:
- Respond to standard prior authorization requests within 72 hours
- Respond to urgent requests within 24 hours
- Provide specific denial reasons that cite the clinical criteria used
- Report prior authorization metrics publicly, including approval and denial rates by service type
- Implement electronic prior authorization for at least some services
These are real requirements with real penalties for non-compliance. CMS has signaled it will enforce through plan audits and contract actions.
What the rule does not do
It does not eliminate prior authorization. It does not guarantee approval. It does not shorten payment timelines.
A plan can deny a request within 72 hours just as easily as it can approve one. The rule regulates speed and transparency, not outcomes. A fast denial with a cited reason is still a denial.
The rule also does not apply to commercial insurance. If your payer mix includes significant commercial volume, those plans operate under different rules and different timelines.
The transparency piece matters more than the speed
The requirement to report approval and denial rates by service type is the sleeper provision in this rule.
For the first time, practices will have access to data showing which plans deny which services at what rates. This is actionable intelligence. If Plan A denies 40% of imaging requests and Plan B denies 8%, that is not just a billing issue. It is a payer mix issue.
Practices that track this data and adjust their payer mix, contract negotiations, or service line decisions accordingly will have an advantage over practices that do not.
The 72-hour window is not the constraint
Here is the practical reality. The 72-hour response window applies to the plan's decision on the authorization request. It does not apply to:
- How long it takes your staff to prepare and submit the request
- How long the plan takes to process the claim after authorization is approved
- How long the plan takes to pay the claim after processing
The total timeline from patient visit to payment still includes your internal workflow, the authorization decision, claim submission, claim processing, and payment release. The rule addresses one segment of that chain.
What practices should do before July 1
Audit your current prior auth workflow. Time how long it takes from clinical decision to submission. Identify bottlenecks. The plan's 72-hour clock starts when they receive the request, not when you decide you need one.
Review your top payers' auth requirements. MA plans are updating their processes to comply. Some are ahead of the rule. Some are scrambling. Know where your top 5 payers stand.
Set up tracking for denial reasons. The rule requires plans to cite specific clinical criteria. Start capturing those citations. Over time, you will see patterns that tell you which services trigger scrutiny and which plans are outliers.
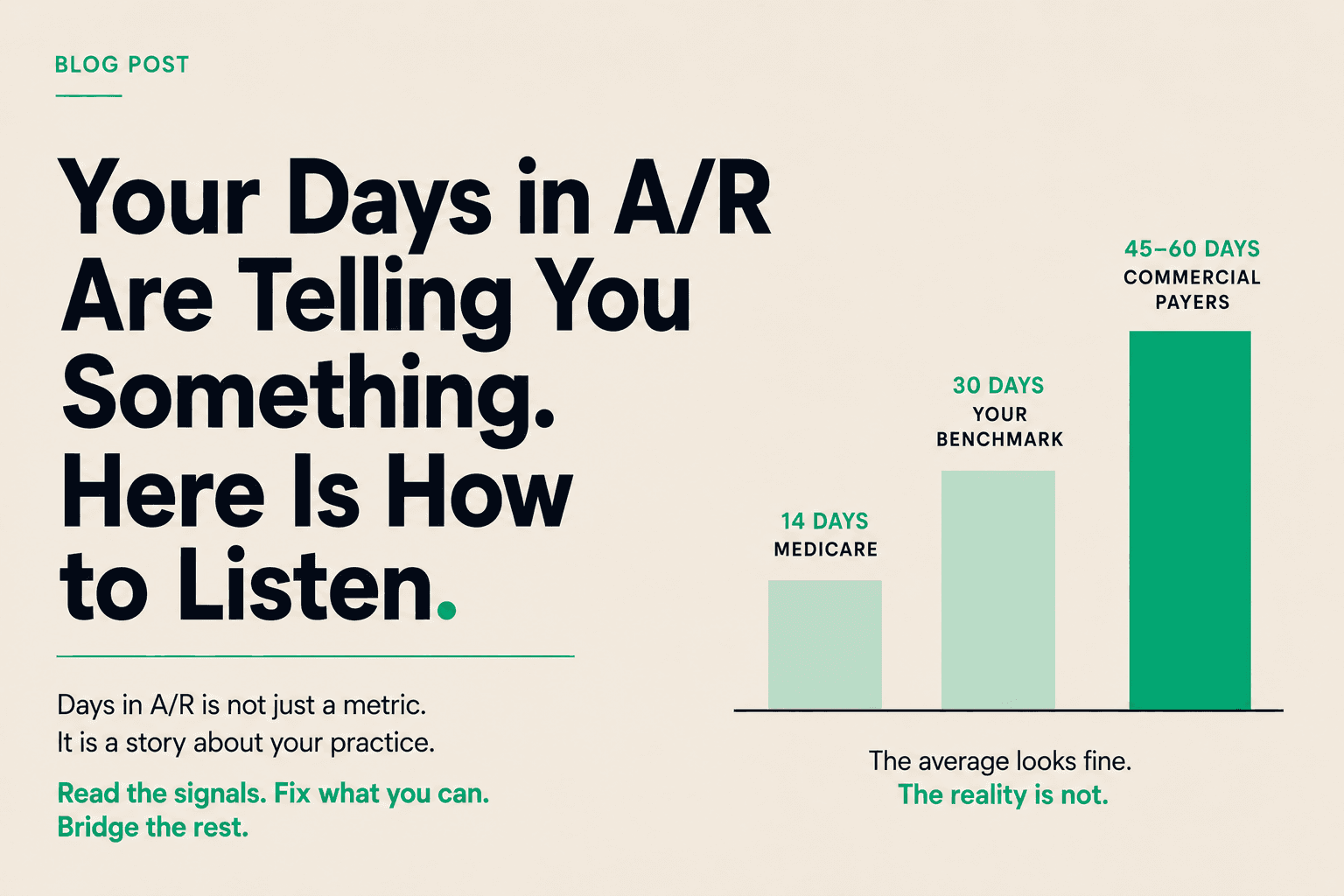
Do not expect cash flow relief. The rule may reduce some administrative friction. It will not change the underlying payment timeline. If your practice is waiting 45-60 days from claim submission to payment, that timeline is unaffected by prior auth reform.
The Copay take
Prior authorization reform is real progress. It is also incremental progress that addresses one symptom of a larger structural issue.
The structural issue is the gap between delivering care and getting paid. That gap is 30-60 days for most practices, longer for some specialties and payers. Prior auth is one contributor. Payment processing timelines, claim review queues, and denial appeals are others.
The practices managing this best are not waiting for regulatory relief. They are treating their submitted claims as working capital and accessing that capital on their own timeline.
If the July 1 rule changes your auth workflow, good. But do not mistake workflow improvement for cash flow improvement. They are related, not the same.
The bottom line
Healthcare receivables financing is a tool. Like any tool, it works best in the right context. If your practice has solid operations, predictable claim volume, and a cash flow gap created by payer timing rather than operational problems, it is worth exploring.
If you want to run the math on what your days in A/R is costing you and whether receivables financing makes sense at your volume, Copay is a good place to start.