Your Days in A/R Are Telling You Something. Here Is How to Listen.
Written by Emily Davis
Your Days in A/R Are Telling You Something. Here Is How to Listen.
Most practice owners know their days in A/R number. Fewer know what it is actually saying.
Days in A/R is not just a metric. It is a story about how your practice interacts with the payment system. The number tells you about payer behavior, claim quality, staff efficiency, and patient mix. But only if you know how to read it.
What days in A/R actually measures
Days in A/R measures the average number of days it takes to collect payment after a claim is submitted. The calculation is simple: divide your total accounts receivable by your average daily charges.
If you have $1.2 million in A/R and average $40,000 in daily charges, your days in A/R is 30. That means, on average, it takes 30 days from claim submission to payment.
The MGMA benchmark for primary care is around 30 days. For specialties, it varies. Surgical practices often run higher because of complex coding and prior auth requirements. Radiology can run lower because of high volume and cleaner coding.
Why the benchmark is misleading
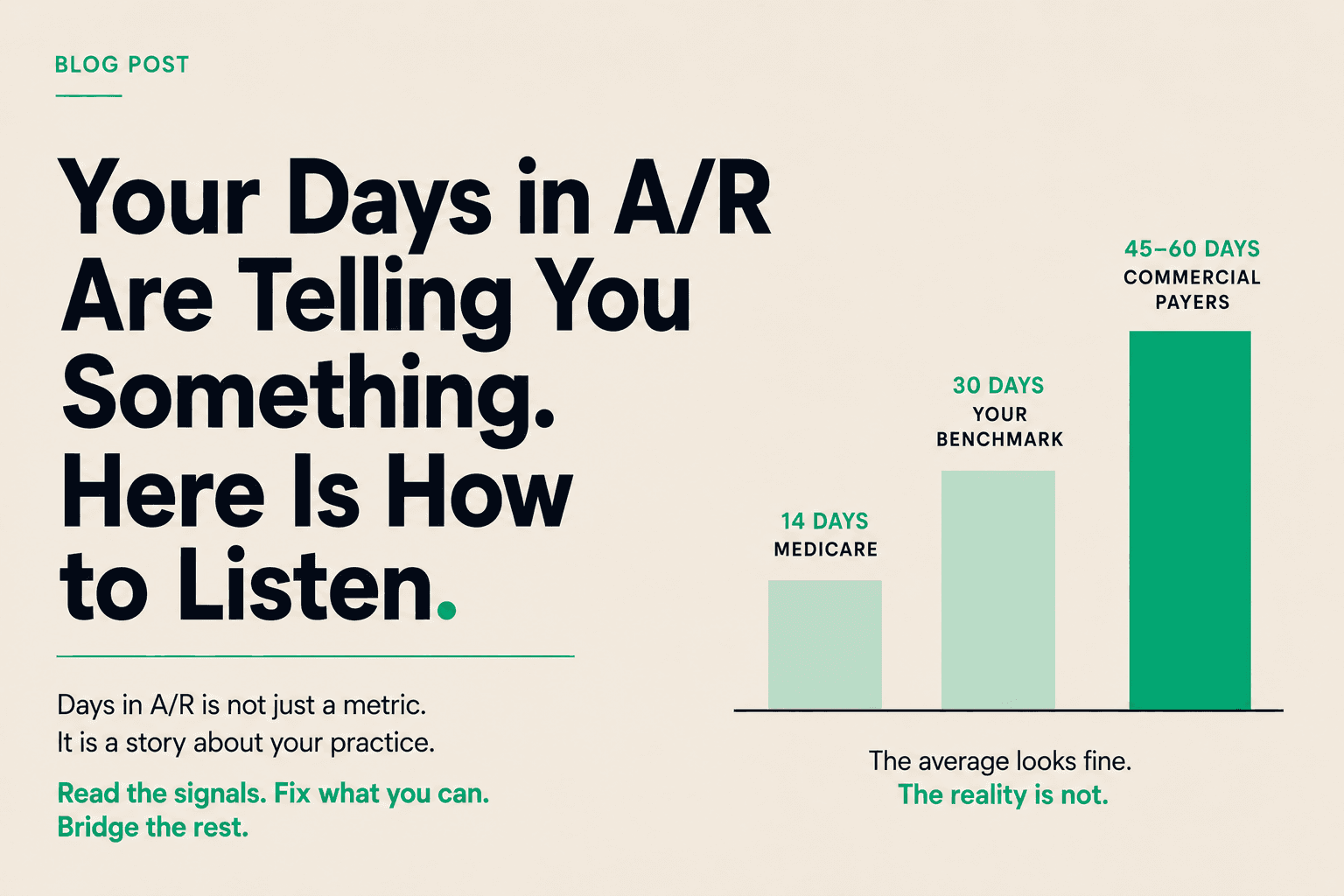
The 30-day benchmark is an average. It blends fast payers and slow payers. It blends clean claims and denied claims. It blends Medicare, which pays in 14 days, with commercial payers that take 45 to 60 days.
A practice with a 30-day average might have Medicare claims paying in 14 days and commercial claims sitting at 60 days. The average looks fine. The reality is not.
The better way to read days in A/R is to segment it. Break it down by payer. Break it down by claim age. Look at what percentage of your A/R is over 90 days. That number tells you about claim quality and follow-up discipline.
The 90-day threshold
Claims over 90 days old are a red flag. At that point, the probability of full collection drops significantly. Some payers have timely filing limits. Some claims have been partially paid and the balance is sitting in a queue nobody is watching.
A healthy practice keeps 90-day A/R under 15% of total A/R. If you are running higher than that, the problem is not payer speed. It is your internal process.
What drives days in A/R up
Several factors push your number higher:
Claim errors. A claim with a coding error, missing modifier, or incorrect patient information does not get denied immediately. It sits in a queue. It might take 30 days to get a denial, then another 30 days to resubmit and reprocess.
Prior authorization gaps. Services that require prior auth but do not have it at the time of billing get held. Sometimes they get denied. Sometimes they get pended. Either way, the clock keeps running.
Payer-specific delays. Some payers are consistently slower. If your payer mix shifts toward slower payers, your days in A/R goes up even if your internal process is perfect.
Patient responsibility. High-deductible plans mean more patient responsibility. Patients pay slower than insurers. If your front desk is not collecting at time of service, your A/R gets longer.
How to improve it
The fixes are operational, not financial.
Front desk verification. Verify eligibility and benefits before the visit. Collect copays and deductibles at check-in. Every dollar collected at the front desk is a dollar that does not enter your A/R.
Clean claim rate. Aim for 95% or higher. That means coding accuracy, complete documentation, and correct patient information on first submission. Every rejected claim adds 30 to 60 days.
Denial management. Track denials by reason. Fix the root causes. If you are getting denials for missing modifiers, train your coders. If you are getting denials for timely filing, fix your workflow.
Payer-specific follow-up. Know your payers. Know their timelines. Know their portals. Assign staff to follow up on claims before they hit the 90-day mark.
When operational fixes are not enough
Even with perfect operations, the gap exists. Medicare pays in 14 days. Commercial payers take 30 to 60. Some take longer. Your payroll, rent, and supplier invoices do not wait.
That is where healthcare receivables financing comes in. It does not replace good billing operations. It complements them. You run a tight ship on the front end. You use receivables financing to bridge the gap on the back end.
At Copay, the rate is 0.75% for the first 10 days, with a daily rate after that. No minimums. No contracts. You access capital tied to specific claims, at the claim level, and reconcile when the payer settles.
The bottom line
Days in A/R is a diagnostic tool. It tells you where to look. If your number is high, segment it. Find the payer, the process, or the people driving it. Fix what you can fix.
Then bridge the rest. The gap is structural. You do not have to wait in it.
If you want to run the math on what your days in A/R is costing you and whether receivables financing makes sense at your volume, Copay is a good place to start.