Denials Are Not Free: The Real Cost of Every Rejected Claim
Written by Emily Davis

Denials Are Not Free: The Real Cost of Every Rejected Claim
A new AHA report pegged the total cost of chasing insurance denials, prior authorizations, and documentation disputes at $43 billion in 2025. Across all providers. That number is so large it becomes abstract.
Here is a more useful number: what does a single denied claim cost your practice?
Most owners think the answer is "the cost of the claim, if we eventually don't collect it." But that is not the right calculation. The real cost of a denial includes the time to identify it, the staff hours to work it, the resubmission cycle, the cash sitting frozen during the appeal, and the claims that never get worked at all because your billing team has capacity limits.
When you run that full accounting, a $200 denial costs a lot more than $200.
The four costs of a denial
Time to identify. Clean claims that pay on first pass show up in your remittances and close out. Denied claims require someone to catch them, read the reason code, and decide what to do next. On a busy billing team, this discovery lag can run two to four weeks. During that time, the claim is aging and the appeal window is shrinking.
Staff cost to work the appeal. A billing specialist who earns $50,000 per year costs your practice roughly $25 per hour loaded. A denial that requires one hour to research, document, and resubmit costs you $25 in labor before you collect anything. Most complex denials take longer. On a $200 claim, that is a 12.5% overhead before you have accounted for anything else.
The resubmission clock. When you appeal a denial, the payer's payment clock resets. A claim that should have settled in 45 days now goes through a separate review process that can add another 30 to 60 days. Your staff paid. Your supplies were used. Your overhead ran. The payer is now on a second clock that they control entirely.
The claims that fall off the edge. Most billing teams work denials by value. Low-dollar denials get deprioritized. Some never get touched. The industry estimate is that 15 to 20% of denied claims are never reworked. They just age out. That is pure write-off on claims the payer initially chose not to pay.
Add it together. A $200 claim with a denial costs you $25 in labor, adds 45 days to the payment cycle, and has a meaningful probability of never being collected at all. Your actual cost is not $200. It is more like $200 times the probability of collection, minus the labor, minus the cost of the cash lag.
Why clean claim rate matters more than denial management
There are two ways to approach the denial problem. You can build better denial management, or you can prevent denials.
Denial management is reactive. It is staffing and process designed to catch rejections and fight them. It works, and it is necessary. But it is a cost center. Every dollar recovered through appeals was more expensive to collect than a clean claim would have been.
Clean claim rate is proactive. It measures what percentage of your claims go out error-free on the first submission and pay without manual intervention. National benchmarks put the target at 95% or higher. Below 90% and you have a systematic problem, not a random one.
The practical difference: a practice billing $600,000 per month with a 90% clean claim rate is generating 600 denials per month that need to be worked. At $25 per denial in labor, that is $15,000 per month in overhead before considering write-offs or cash flow impact. Improving to 96% clean claims cuts that to 240 denials per month, saving roughly $9,000 in labor costs.
That math is conservative. It does not account for the cash flow impact of faster first-pass payment.
The cash flow layer most practices miss
Denials have a direct cash flow effect that sits on top of the labor cost.
When a claim is denied and enters the appeal cycle, the revenue tied to that claim is frozen. It is neither in your account nor officially written off. It sits in a gray zone where your practice management system shows it as outstanding but your operating account reflects none of it.
For a practice with a 10% denial rate and $600,000 in monthly claims, that is $60,000 per month entering the denial queue. If your average appeal cycle is 45 days, you have roughly $90,000 sitting in denied claims at any given moment. That $90,000 is capital you have earned but cannot access while the appeal resolves.
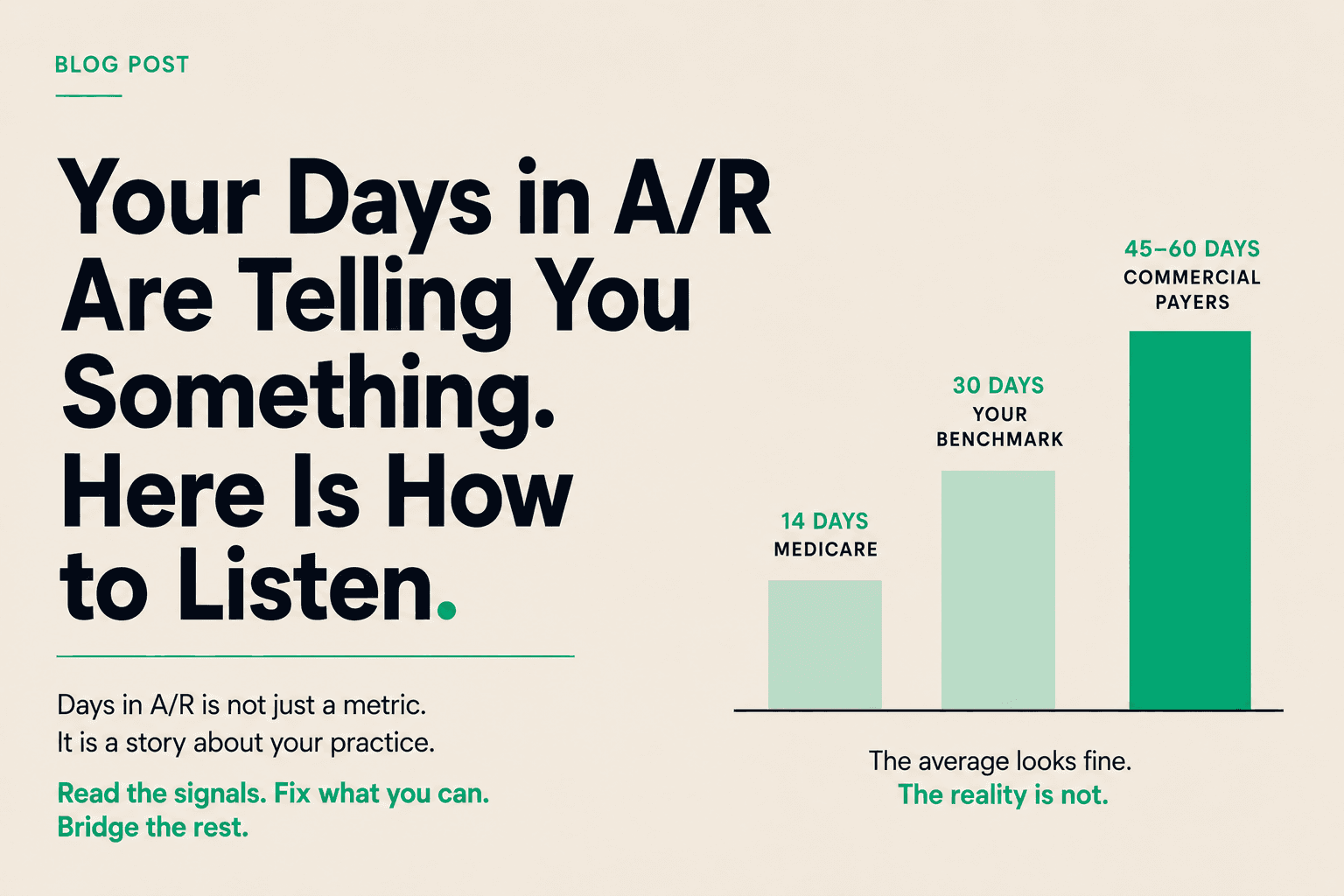
Layers compound. You already have 45 to 60 days of clean claims in your normal A/R pipeline. Denied claims add another 45-day tail on top of that. For the claims that require multiple rounds of appeal, the cash can be frozen for 90 to 120 days.
What to do about it
Measure your clean claim rate by payer. Your overall rate hides variation. A practice with 97% clean claims on commercial payers and 85% on Medicaid is not a 91% practice. It is two different problems with two different root causes.
Audit denial reason codes quarterly. Denial reasons cluster. If 30% of your denials in a quarter are the same code, you have a workflow problem, not a random claim problem. Fix the workflow and you eliminate a category of denials, not just individual claims.
Build a denial value threshold. Not every denial should get the same staff time. Set a clear dollar threshold below which you write off rather than appeal, and above which you always appeal. Mixing high and low-value denials in one queue is how low-value claims crowd out high-value recovery work.
Account for the cash gap while you appeal. This is the piece most practices overlook. You should not have to run tight on operating cash because $90,000 is frozen in your denial queue. That capital exists. It is in transit between a payer dispute and your account.
Healthcare receivables financing works here the same way it works for standard payment lag. You advance against submitted claims at a transparent daily rate, including claims that are in appeal. When the payer settles, the advance reconciles. The denial management process continues. You stop waiting on it.
The bottom line
Denials are not a billing nuisance. They are a capital efficiency problem. Every denied claim represents labor, cash sitting frozen, and a meaningful probability of write-off. The $43 billion figure the AHA reported last month is not an abstraction. It is millions of individual practice decisions about which claims are worth fighting and which will quietly disappear.
The practices managing this well do three things. They optimize clean claim rate so fewer claims enter the denial queue in the first place. They build systematic denial management so the ones that do enter get worked consistently. And they stop treating the cash trapped in denied claims as untouchable while appeals run their course.
Your A/R is an asset at every stage of its lifecycle, including while a denial is pending.