CMS Just Named 29 Early Adopters for Electronic Prior Auth. The Payment Clock Didn't Move.
Written by Emily Davis
CMS Just Named 29 Early Adopters for Electronic Prior Auth. The Payment Clock Didn't Move.
On Tuesday, CMS announced that 29 healthcare organizations have joined its electronic prior authorization initiative as early adopters, building momentum ahead of the 2027 mandate. Cleveland Clinic is on the list. Epic is on the list. Major health plans and physician networks are on the list.
It is genuinely good news. The technology is moving. The infrastructure is being built. And it still does not fix the problem that matters most to the independent practice owner who opens their bank account on Thursday before payroll runs.
Let me explain why, and what else happened this week that is worth paying attention to.
What CMS actually announced
The 2027 requirement will mandate that payers and providers use standardized electronic prior authorization workflows for most Medicare and Medicaid claims. The early adopter program is a voluntary effort to pilot those workflows now, work out the interoperability gaps, and arrive at 2027 with tested systems rather than a cold start.
This is smart policy design. Voluntary adoption before mandated rollout means the hard problems get discovered and solved before everyone is required to use the system at once.
The participating organizations span the full chain: EHR developers like Epic, health systems like Cleveland Clinic, payers, physician practices, and digital health platforms. The goal is end-to-end testing of the authorization workflow so that when a provider requests auth, it moves electronically and quickly through the payer's review process.
For practices in high-auth specialties, this is a real quality of life improvement on the horizon. Requesting authorization for a procedure without faxing, calling, and following up will save staff time and reduce scheduling delays.
But here is the part the press releases do not say out loud.
The authorization clock and the payment clock are separate
Prior authorization is a gate that sits before claim submission. Electronic auth makes the gate open faster. It does not touch what happens after the gate.
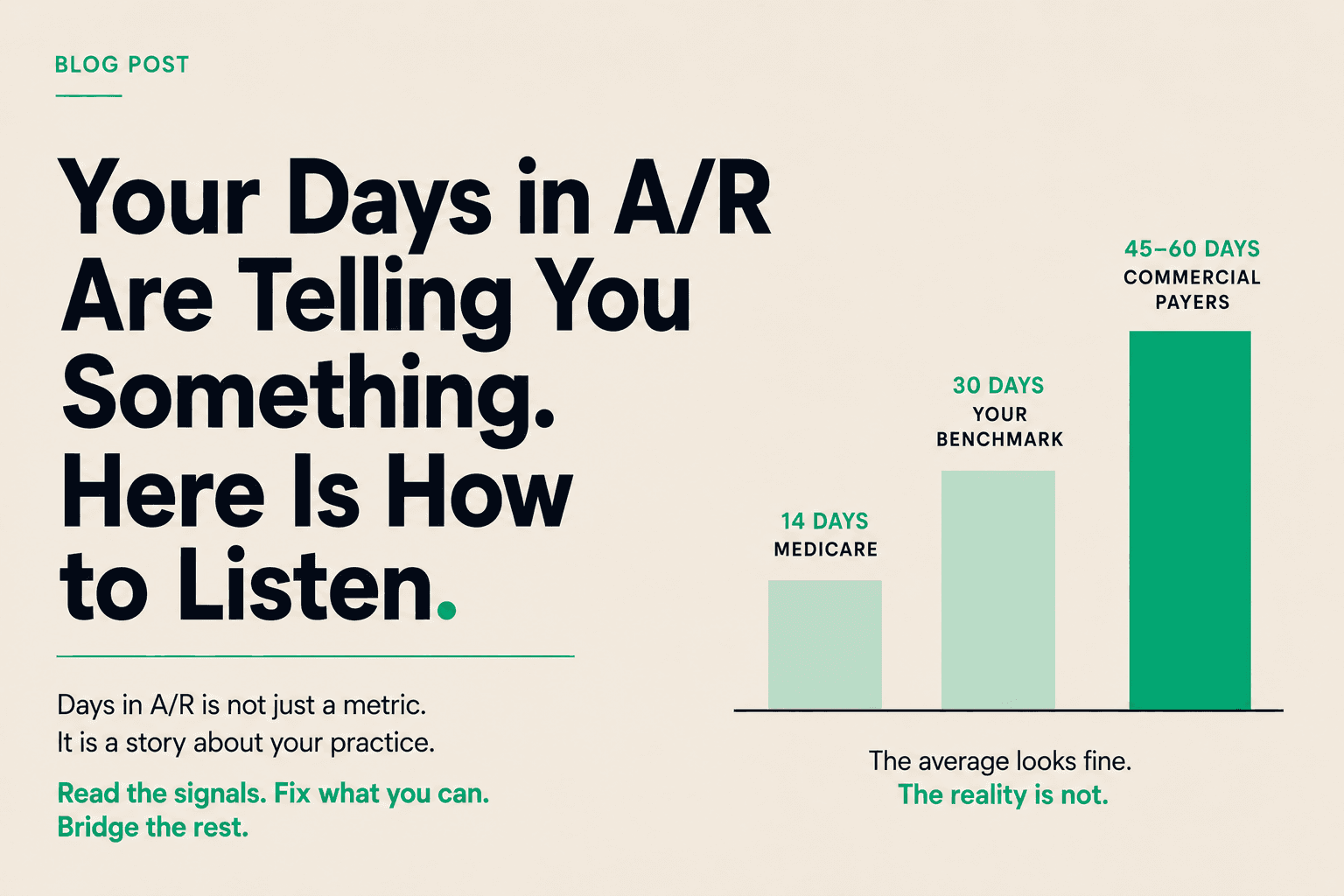
After a claim is authorized and submitted, it enters the payer's payment processing queue. That queue runs on its own timeline, which is not governed by prior auth rules and is not affected by how quickly authorization was obtained. A claim that gets authorized in 24 hours instead of 10 days still sits in adjudication for 30 to 45 days before payment.
The practices that will benefit most from electronic prior auth are those in specialties where auth delays cause the most scheduling disruption. Orthopedic surgery. Cardiology. Oncology. The workflow improvement is real. The cash flow improvement is marginal, because authorization time was never the majority of the payment lag.
This is not a critique of the CMS initiative. It is a description of what it does and does not solve.
The denial data published this week
A Health Affairs study released this week looked at 30% of the Medicare Advantage market and found initial denial rates averaging 17%. Of those denials, 57% were ultimately overturned on appeal.
Read that again. More than half of all initial MA denials are wrong. They are reversed when someone challenges them. The clinical justification for the original denial did not hold up when reviewed.
For independent practices, this creates a specific math problem. If your MA denial rate tracks the national average, about one in six claims is being denied on first pass. Of those denials, more than half will eventually pay, but only after your staff works the appeal, and only after another 30 to 60 days passes while the appeal is reviewed. The claims that never get worked, the ones below the dollar threshold where your billing team writes them off, represent denied revenue that you never collected for work you already did.
The average denial across practice sizes costs around $25 to $50 in billing staff time to work, not counting the cash flow impact of the delay. On a practice with $600,000 in monthly MA claims and a 17% denial rate, that is roughly $100,000 per month entering the denial cycle. Some of it will come back. All of it will come back late. A portion will never come back at all.
The fee schedule pressure that is still building
Separate from the authorization story, the 2026 Medicare physician fee schedule has finalized cuts of 3 to 5% for procedure-heavy specialties. Surgical specialties, radiology, and certain diagnostic services are absorbing reductions while evaluation and management codes remain relatively stable.
The practical implication for specialty practices is that the same volume of work generates less revenue per claim than it did last year. Combine that with a 17% initial denial rate and a 30 to 45 day payment cycle, and the margin pressure on procedure-heavy practices is real and cumulative.
The CMS electronic prior auth initiative will eventually help with scheduling friction in those specialties. It will not offset the fee schedule reductions.
Putting it together
Three things happened this week that are worth tracking as a pattern:
First, CMS is making real infrastructure investments in prior authorization. The technology is improving. The 2027 mandate will bring meaningful workflow change.
Second, the denial data confirms what practice billing teams already suspect: a substantial portion of initial MA denials are not clinically justified. They are workload shifted onto providers who accept the denial rather than appeal it. The practices leaving the least money on the table are the ones appealing systematically.
Third, fee schedule reductions for procedure-heavy specialties are compressing margins on the revenue side while the cost structure stays fixed.
None of this resolves by waiting. Electronic auth will improve over the next 18 months. Denial rates may or may not improve. Fee schedules adjust annually, usually not in the provider's favor. The cash flow gap that results from this structure is a standing feature of healthcare payment, not a temporary problem waiting on a single fix.
The practices navigating this best are not waiting on any particular reform. They understand their days in A/R, they appeal denials systematically, and they treat submitted claims as working capital they can access on their timeline rather than the payer's.